AZT, Nevirapine: Do Anti-Retroviral Drugs Cause AIDS?
Nevirapine has been in the news recently over a study in Africa, where researchers apparently "forgot" to report numerous serious side effects and even several deaths. The study was to prove efficacy in reducing HIV transmission from pregnant mothers to their newborns, but researchers also "forgot" to include a control group of mothers that did not receive the drug. Grave oversights? Apparently the US health authorities thought so, because the application by Boeringer Ingelheim to use their drug on pregnant mothers in the US was never approved. Toxicity seems to be severe, but it was not properly reported, and could not be compared to non-toxic alternatives.
Studies for the approval of AZT were similarly defective. Indeed, AZT had been developed in the 60's as a chemotherapy drug and shelved because of ... toxicity problems. It was taken out of mothballs, so to speak, when an extraordinary media frenzy and predictions of doom for mankind at the hands of the pandemic demanded an immediate "cure for AIDS". For more data on AZT, see here and here.
Now why would we "treat" an immune weakness with highly toxic drugs? HIV, a new type of "retrovirus" was announced by Robert Gallo at a press conference, and we needed an immediate killer drug. In a pattern similar to the Nevirapine story, the virus itself was postulated as the culprit, but the virus isolation is highly contested. Gallo "forgot" to let the scientific community in on his secret. Anyway, the "virus" was painted as the culprit by a press campaign and the heavy toxic drugs were brought in, without toxicity testing, because "people were dying" and "the pandemic" was "going to wipe out mankind" if something was not done immediately.
But what about all the people that test HIV positive? Apparently, they test positive to something else than the virus. The HIV test was developed for blood screening and is, according to manufacturers, not a test to indicate the presence of a virus. No one has yet claimed a £ 1000 cash prize for proving HIV isolation in a scientific publication.
Some days ago, I was checking out Jon Rappoport's www.nomorefakenews.com and came across an interesting discussion - you can find a copy at the very end of this article. Rappoport was one of the first skeptical inquirers who came out with a book (AIDS INC) questioning the science behind the HIV/AIDS Gordic knot. Rappoport, upon investigation, concluded that HIV is not the cause of AIDS.
Neither are HIV tests specific to indicate the presence of a virus. They react positive to a host of non-HIV-related conditions. Neville Hodgkinson writes about Nevirapine - see his article, as published in The Business below. Hodgkinson says about the AIDS test:
Scores of conditions, including pregnancy itself, as well as infections such as TB that are especially prevalent in Africa, have been shown to affect the immune system in ways that cause positive reactions with test kits used to diagnose “HIV” infection, but have nothing to do with HIV.On the other hand, Boyd Graves tells us that HIV is part of a US government plot to develop an ethnicity-specific bio-weapon. Graves has put together a lot of research on the existence and the activities of a classified "special virus program" and he contends that HIV is the upshot of that program and is used in a genocidal campaign to wipe out blacks.
Let's put two and two together: The balance of evidence tells us HIV is likely not the cause of AIDS. People are dying of AIDS, especially in Africa. Africans are not even tested for HIV before being treated, but large numbers are given the toxic antiretrovirals, because they have symptoms of disease. Africans are starving and living in dangerous sanitary conditions. Many don't have either clean water, sanitation or sufficient food. What is our response? We're sending more antiretroviral drugs to Africa. We are giving those same drugs to pregnant mothers in Africa to "prevent HIV transmission".
What if we were guilty of committing genocide with toxic anti-retrovirals?
If you're interested in more, here is Neville Hodgkinson's article on Nevirapine and Jon Rappoport's excellent "THE LOGIC OF AGENDA".
- - -
The Business, 30/31 January 2005
Fresh cause for concern over the side-effects of nevirapine
Doubts emerge over clinical studies of crucial HIV drug
By Neville Hodgkinson
A tragedy of global proportions is unfolding over a toxic anti-HIV drug given to hundreds of thousands of women and babies in the developing world in the belief that it can help prevent the spread of Aids.
The drug, nevirapine, has become so central to Aids agencies’ efforts to support African and other developing nations that they are defending its use in dozens of poor countries, despite evidence that flaws in claims for its safety and effectiveness were covered up at the highest level by government scientists in the United States.
Nevirapine is acknowledged by Boeringer Ingelheim, its German manufacturer, to be capable of causing severe liver damage and life-threatening skin reactions soon after patients start taking regular doses. This month a new warning about its dangers was issued by US health officials. Deaths have been reported from several countries.
But a study published by The Lancet in 1999 purported to show that when given as a single dose to HIV-positive mothers at delivery, and to the babies within three days of birth, the drug safely reduces transmission of HIV from mother to child.
The study was initiated and funded by the powerful Division of Aids of the National Institute of Allergy and Infectious Disease (NIAID), part of the American Government’s massive National Institutes of Health (NIH) complex at Bethesda, Maryland. The research, conducted on maternity wards in Kampala, Uganda, was led by investigators from Johns Hopkins University, Baltimore, Maryland. The findings were hailed by Dr Anthony Fauci, NIAID’s director, as opening up “an entire new avenue” towards prevention of transmission of HIV in countries that could not afford more expensive drugs.
To help get nevirapine established for this purpose, Boehringer Ingelheim offered to provide it free for five years to government hospitals in developing countries. Along with the drug’s endorsement by the World Health Organisation and the Joint United Nations Programme on HIV/AIDS (UNAIDS), this gave Aids organisations a powerful tool for pressing for its rapid introduction and there are now 122 programmes administering the drug in 57 developing countries. The product, which is also used as part of some anti-viral “cocktail” treatments for Aids patients, has today become the company’s sixth best-selling drug with sales totalling E310m ($412m, ₤217m) in 2003.
On 19 January, the US Food and Drug Administration (FDA) warned that cases of liver damage were more common with nevirapine, especially in women, than with other anti-HIV drugs. Some instances have been fatal, including in pregnant women. The FDA said doctors should weigh benefits and risks before prescribing the drug, adding that no serious toxicity or deaths have been reported with the single-dose treatment. The drug is not licensed for this use in the US or Europe.
In July 1999, even before the Uganda study results had been published, Boehringer Ingelheim asked South Africa’s Medicines Control Council (MCC) to fast-track approval of the single-dose regime in mothers and babies. When South African authorities insisted it was not proven safe and that caution was needed, massive criticism followed from within and outside the country.
Worldwide media derision was directed particularly against South Africa’s president, Thabo Mbeki, who had questioned the relevance of Western approaches to Aids, particularly in the African setting, arguing that poverty and malnutrition were the real causes of immune deficiency there.
The push behind nevirapine was one of the most extensive promotional drives by the world’s media for a pharmaceutical product, perhaps surpassed only by the way NIAID catapulted AZT, the first purported anti-Aids drug, onto world markets through studies that were also shown subsequently to be deeply flawed. Manufactured by Burroughs Wellcome (a company now subsumed in GlaxoSmithKline), AZT was said to be the “gold standard” of Aids treatment until the biggest and longest trial, conducted jointly by French and UK government researchers, showed more deaths in patients given the drug early than in “controls” who received it later.That finding was also downplayed and AZT survived, becoming used in much smaller doses as part of the “cocktail” treatments. AZT is also given to pregnant mothers and their babies for the same purpose as nevirapine; it was in comparison with AZT that nevirapine was declared to halve the risk of transmission of HIV in the Uganda study, from 25% to 13%.
Yet some scientists argue that AZT is useless and dangerous. They say that although nevirapine and AZT can reduce the proportion of babies who test HIV-positive, this may simply be a result of general suppression of the immune system by the drugs. Scores of conditions, including pregnancy itself, as well as infections such as TB that are especially prevalent in Africa, have been shown to affect the immune system in ways that cause positive reactions with test kits used to diagnose “HIV” infection, but have nothing to do with HIV.
This interpretation is supported by a follow-up study in the Uganda trial showing that despite the halving of HIV-positivity attributed to nevirapine, 18 months later the overall death rates among the babies did not differ significantly between the AZT and nevirapine groups. The death rates were also extremely high, averaging 12%.
Furthermore, the Uganda trial had no drug-free group of subjects to compare with the treated groups, even though other studies have shown “HIV” transmission rates below 13% when untreated.
In January 2001, South Africa’s MCC yielded to pressure from Aids campaigners and granted Boehringer Ingelheim a provisional licence for mother and baby treatment in South Africa, based on the single Lancet study.
Problems began to surface however in 2002, after the manufacturer applied to the FDA for a licence to sell the drug for the same purpose in America. The Uganda study was central to the application; but an audit of the findings showed problems, including differences of opinion between the American researchers and Ugandan hospital staff over what constituted “serious adverse events” in the trial subjects. When investigators asked for the original case files, trial overseers were unable to produce most of them.
In March 2002 the company withdrew its application, citing “questions regarding reporting and documentation” in the study. Dr John LaMontagne, deputy director of the NIAID, reassured the press that “there is no question about the validity of the Lancet study … the problems are in the rather arcane requirements in record keeping.”
Last month, Associated Press, the American news service, reported that top NIH officials, including Fauci, had been warned by an audit team that the study may have under-reported severe adverse events among the trial subjects, including at least 14 deaths. Researchers had also acknowledged that “thousands” of adverse events were not reported.
Boehringer Ingelheim, in a pre-audit check of the trial, found incomplete safety data and arbitrary definitions of severity of adverse events in patients, compounded by the fact that the investigators were “not actually seeing the patients whose events they are evaluating.” A 16-page report on these findings, faxed to the NIAID’s Division of Aids, was marked by one of the division’s officials “Sensitive information. Asked for it to be destroyed when audit is upon us.”
Other documents showed how NIH chiefs downplayed and delayed reporting the problems, fearing the potential impact on the drive to extend the use of nevirapine. In particular, Fauci and Dr Edmund Tramont, head of the Division of Aids, were concerned not to jeopardise a $500m mother and child HIV prevention initiative for Africa, announced a few weeks later by President Bush, specifically to support the nevirapine roll-out.
In March 2003, Tramont released a report on a Division of Aids re-evaluation of the Uganda study, again asserting that the study’s overall conclusions on safety and effectiveness were reliable. But Tramont excluded from this report the findings of an expert panel that had specifically reviewed the data on safety and which concluded that the safety claims in the original study could not be validated. The panel drew attention to lack of adherence to serious adverse event reporting requirements, poor quality of subject records, a failure of study staff to use proper toxicity grading scales, and absence of staff supervision and quality control.
Tramont’s report also appears hard to reconcile with the findings of an independent audit of the study contracted previously by NIAID which found a “large number of infants with apparent failure to thrive past six months of age”; and that some and perhaps many infants had serious health problems at 12 months, suggesting “more pathology than had previously been reported.”
In July 2003, NIH appointed Dr Jonathan Fishbein, an expert on drug safety and development, to develop and oversee standards of conduct in clinical research in the Department of Aids through a newly-created post, Director of the Office for Policy in Clinical Research Operations. Before his appointment, Fishbein was vice president of North American Medical Services at Parexel International, one of the largest contract research organisations in the world.
Four months into the job, Fauci presented him with a certificate expressing appreciation of his “outstanding contributions and efforts in support of the NIAID mission”. But thereafter, things began to sour. “It soon became apparent that I was hired not so much to change things at DAids [Division of Aids] but to give the appearance that I was,” Fishbein told Anthony Brink, a South African lawyer who has for several years been chronicling the nevirapine story (see www.tig.org.za).
After persistently trying to see the irregularities he had uncovered addressed within the Division of Aids, Fishbein was sacked. Unable to interest other NIH departments, or the Department of Health and Human Services that is responsible for NIH, he took his concerns to the US Congress. Officials of the Subcommittee on Oversight and Investigations of the Energy and Commerce Committee took him seriously; they agreed with NIH a new review of the Uganda study, to be conducted by the Institute of Medicine. But the review is charged only with assessing the integrity of the data and will not address issues of scientific misconduct, cover-up, or reprisal.
In testimony submitted to the inquiry earlier this month, Fishbein says it quickly became apparent to him “that something did indeed go terribly wrong” with the Uganda study. His statement tells of “an atmosphere of intimidation” perpetrated by the Division of Aids leadership, especially towards its regulatory affairs branch; and of how NIAID officials “have conspired, and continue to conspire, to hide from the public serious deficiencies” in the Uganda trial that would otherwise invalidate its results.
Those deficiencies included poor record-keeping and lack of follow-up on adverse events, suggesting that “the care of study subjects was not sufficiently overseen by the study staff and jeopardised the safety of the subjects given this potent drug’s known serious and potentially life-threatening side effects.”
To date, Fishbein’s whistle-blowing efforts appear to have failed to shift opinion among leading Aids scientists, drug activists and their media supporters, who are so deeply convinced drugs are the way to prevent the spread of Aids that they regard the controversy as threatening lives.
One American journal, Science, said in its December 24 issue that the revelations had dismayed Aids researchers and clinicians around the world. It quoted Dr Clifford Lane, NIAID’s deputy director, as worrying that the story “may cause people to stop using nevirapine”, so that “infants could be infected and die needlessly.”
A report from Washington in the UK science journal Nature, headlined “Nevirapine trial was not flawed, say researchers”, quoted the doctor-president of Global Strategies for HIV Prevention as declaring: “There are already mothers who are refusing to take nevirapine. This is the most successful therapy in the entire Aids epidemic. It should not be attacked.”
Nature said scientists and patient advocates had united to defend the treatment, pointing out that trials in South Africa, Malawi and Thailand have confirmed nevirapine’s safety and effectiveness. But in July 2003 South African drug regulators withdrew nevirapine’s provisional licence for perinatal use, citing “data integrity” problems in the Uganda study.The Malawi trial cited is not comparable with the Uganda one, and shows quite different results: a reported transmission rate of 20.9% in babies who received nevirapine, and 15.3% in babies who received nevirapine and AZT together.
Furthermore, the conduct of this study, also led by Johns Hopkins researchers, has been challenged by staff working at the Zomba Central Hospital, one of the trial sites. Dr Peter Safar, head of the department of Obstetrics and Gynaecology, and Dr Christian Fiala, an Austrian gynaecologist and long-standing critic of the theory that immune deficiency in Africa is caused by HIV, wrote to the South African Medical Journal in 2002 protesting that the organisers had “ignored the most basic principles of research in medicine”.
They said the deficiencies included a lack of proper information and counselling over HIV testing, failure to inform the women of possible side-effects and refusal to tell doctors and nurses on the wards which drugs their patients were receiving.
Article by Jon Rappoport - www.nomorefakenews.comTHE LOGIC OF AGENDA
FEBRUARY 6, 2005. More and more, as America and other countries sink into a morass of dumbness based on a stark lack of education in schools, people emerge from adolescence with a compelling sensation that they must take up the sword on various issues based on a twitch, an agenda, an obsession, an overriding feeling.
In other words, any attempt at being rational is trumped by one's own agenda.
I encountered this as I researched my first book (1988) called AIDS INC. Halfway through the project, I realized that the central issue was: does HIV really cause AIDS?
There was a whole lot riding on this question.
As I accumulated more and more evidence to support a resounding NO, I ran into people who were riding into the debate on their own personal donkeys.
There were people who felt that the future of the world was under an ominous cloud called bio-war devastation. For them HIV was just another illustration that we were all doomed by artificially created germs. HIV was made in a lab and it was killing millions.
There were people who believed that gay men had been singled out for a holocaust. Therefore, HIV was the means to this end.
There were people who believed that gay men were being blamed for AIDS, but the exonerating discovery of HIV proved that AIDS was really a neutral epidemic that favored no group.
There were people who believed that eating animal flesh was a crime and a cause of widespread disease, and therefore HIV was of no consequence.
There were people who believed that vaccines were death makers, and "therefore" HIV (a prime killer) must be hiding in smallpox vaccines.
There were people who believed that hemophiliacs were dying at a much higher rate, and therefore HIV must be the contaminant in blood factors these patients were injecting.
There were people who believed that genocide in Africa was ongoing, and therefore HIV must be the tool.
There were people who believed that heroin addicts were on a "kill-list," and therefore HIV must be the germ intentionally transmitted through shared needles.
There were people who believed that death was descending on Earth from space in the form of inter-galactic viruses, and an analysis of HIV would prove it was an off-planet germ.
There were people who believed that the medical research establishment was a very reliable source of information, and therefore HIV must be the cause of AIDS.
There were people who believed that heroic breakthroughs were occurring every day in lab germ research, and therefore HIV must be the cause of AIDS.
You get the picture.
I'm not criticizing these initial beliefs. I share some of them.
I'm pointing out that the beliefs can become overriding agendas that then conveniently meld with what is taken to be "a case in point." In this instance, HIV.
You absorb a general idea, decide it's true, and then use it as a magnet to attract specifics.
You come to the conclusion that THIS IS HOW LOGIC IS SUPPOSED TO WORK, because you've never learned otherwise.
Well, this is not how logic works.
Here is another example that widens the view even further. Because CBS screwed up its handling of documents relating to Bush's military service, Bush was, in fact, innocent of any wrongdoing.
Because Eli Lilly documents proving the company knew that Prozac was dangerous were not, in fact, held back from the 1994 trial of Joseph Wesbecker, Lilly was innocent of any wrongdoing.
Because Iraq was not a democracy, the war against the people of Iraq was justified, despite the fact that many reasons given for going to war were shown to be based on lies.
Because many of the people who framed the US Constitution were slaveholders, the document itself could have no value as a political statement. Reading it and finding out what it specifically states would be a complete waste of time.
Because the human genome has now been mapped, we can assume that every human trait and behavior is determined by gene structure.
These linkages and therefores are all invalid.
The initial premises may be right or wrong. But there is a very big swamp that looms when the inferences are drawn from the premises.
Here is another one. Because oil is running out, we are basically doomed. In this case, there is a subliminal argument. NO OTHER FORM OF ENERGY WILL BE UTILIZED IN TIME. Whether you think oil is running out or not, the idea about other forms of energy is really a separate matter. To say that we'll never shift from oil to alt. energies is actually about courage and will and ingenuity and such qualities. The shift does not have to do with the potential availability of alt. energies. In 1870, it would have been easy to say that nuclear energy was a science-fiction fantasy.
Take this argument. All cars are red. I have a car. Therefore, it is red. That's a completely valid inference. Of course, the first premise is untrue.
Or this. There is an ongoing attempt to depopulate Africa. HIV is a germ said to cause death. Therefore, HIV is the major tool being used to destroy Africa. Although I won't try to make a case here to support the truth of the first premise, suffice it to say I believe it is true. The second premise is obviously true. HIV IS being touted as a cause of death. But the inference from these two premises is invalid. Way off the mark. And what takes all this out of the realm of the merely academic is this: suppose the real genocidal effort in Africa is being forwarded by means other than HIV. We'd better find out what those means are. We'd better see the truth.
When logic is not available to people and opinions are everywhere, mind control is in full force. People look exclusively to agendas for answers. And what they find are ideas that lead to dead ends. And the bad guys win. By distraction. By diversion. By lies.
End of article by
JON RAPPOPORT www.nomorefakenews.com
- - -A contribution by Beldeu Singh - March 2006:
CAN I HAVE MY CHEMO SUPPLEMENT PLEASE!Beldeu Singh
The future is wirtten in emerging history. As it is emerging and slowly creeping upon us, we find medical associations banning doctors from prescribing natural antioxidants and micronutrients as supplements to restore health in favor of pharmaceutically prescribed drugs that are not part of the normal and healthy biochemistry of cells but rather can be detrimental to that very life-giving biochemistry and biochemical pathways and we find toxic poisons like AZT that could not be approved for chemotherapy due to its extreme toxicity being presented as a retoviral in conditions like AIDS that is associated with malnutrition and attendant oxidative stress that impairs health rather than a virus proven through the gold standard. Coversely, within this scenario, one should expect toxic chemo being repositioned in the market as a retroviral. That naturally broadens the market and fattens the bottomline.And it has already happened! .... "Since the mortality from H5N1 infection is high, and there is concern that the virus could cause a pandemic, novel treatments for human beings are warranted", Henter said in his hypothesis published online by The Lancet medical journal. There are scientists who believe that "a chemotherapy treatment given to patients with an immune system disorder may work for human avian influenza..." The chemotherapy drug etoposide, which helps kill excess immune cells is the basis for the treatment for an illness known as haemophagocytic lympho-histiocytosis (HLH) because there are clinical similarities. Many disease conditions today are not like scurvy, typhoid, beri-beri, TB or malaria.
Many conditions are caused by free radical initiated reactions in the body by the prolonged use of recreational drugs, toxic drugs, toxic ingredients in cosmetic products or pesticides or fuels and "medicinal" drugs. It is OK to treat conditions like immune disorders that may be caused by free radical damage to biochemical pathways or signaling mechanisms with toxic drugs that (generate free radicals in the body) and could cause similar damage or collateral damage in other systems or cause endothelial dysfunction and the excess NO could interfere with signalling biomolecules.
Medical science, as it presents itself today, is largely a treatment science wherein disease conditions are to be treated with drugs having abondoned health science which is about restoring health through biomolecules that promote and restore cellular function. This chronic deviation is slowly and progressively repositioning toxic drugs and chemicals as clinically useful and later on as harmless or even beneficial for people who have not yet developed any symptoms. As a strategy, toxic drugs appear to be moving in that cycle and AZT is a good example that has dogmatic support.
"Mothers who received the long AZT treatment had a higher rate of stillbirth (8% vs. 4%), severe anemia (7% vs 4%), infection or other HIV events (20% vs 17%), events related to pregnancy or delivery (24% vs 17%) than mothers who received the short course, although fewer died (3% vs 8%)" (Lallemant M et al. A trial of shortened zidovudine regimens to prevent mother-to-child transmission of human immunodeficiency virus type 1. NEJM. 2000 Oct 5;343(14):982-91)."Infants with early positive HIV-1 cultures demonstrated a notable decrement in neurodevelopmental functioning within the first 30 months of life. They achieved motor developmental scores that were increasingly and significantly discrepant [worse] both from the average and from scores achieved by late HIV-1-positive children over the course of the study period" (Smith R et al. Timing of perinatal human immunodeficiency virus type 1 infection and rate of neurodevelopment. Pediatr Infect Dis J. 2000;19:862-71).
"The UK's Committee on Safety of Medicines has issued a warning to doctors about the risk of mitochondrial dysfunction in infants" (Perinatal AZT: New warning on potential risk to infants. www.aidsmap.com. 1999 Jul 21).
"The data show that AZT crosses the human placenta and becomes rapidly incorporated into DNA of placental tissue in a dose-dependent fashion, suggesting that even short exposures to this drug might induce fetal genotoxicity and might also inhibit maternal-fetal viral transmission" (Olivero OA et al. 3'-azido-3'-deoxythymidine (AZT) transplacental perfusion kinetics and DNA incorporation in normal human placentas perfused with AZT. Mutat Res Fundam Mol Mech Mutagen. 1999 Jul 16;428(1-2):41-7). Yet it is precribed as a medicine to pregnant mothers and infants!
"AZT can be severely toxic, and there is compelling evidence that the drug probably doesn't help infected people live longer unless they already have full-blown AIDS ... AZT clearly isn't a very effective anti-AIDS drug" (Cohen J. Fulfilling Koch's Postulates. Science. 1994 Dec 9;266:1647). Yet, there is a dogmatic medical fraternity that insists on AZT as a necessary medicine!
There are many studies that show the extreme toxicity of AZT on blood and bone marrow, in promoting cancers, liver dysfunction and on mitochondria leading to fatigue, muscle wasting and suppression of the immune system. All of these are characteristic of a poison that generates a large number of free radicals in the body. It causes anaemia in all mammals. Its medium term use could certainly suppress and weaken the immune system sufficiently to open the body to opportunistic infections - just like in AIDS! Yet it is a medication!.
"The following is a list of some of the serious adverse reactions to AZT that have been observed in infants, children, and adults who took AZT for certain periods of time. It tells the story of the suffering of patients treated with AZT. These reactions include:Neutropenia, granulocytopenia, anemia, thrombocytopenia, myopathy and myositis,
hepatomegaly with steatosis, hepatitis, pancreatitis, lactic acidosis, sensitization reactions, hyperbilirubinemia, vasculitis, abdominal pain, back pain, body odor, chest pain, chills, edema of the lip, fever, flu syndrome, hyperalgesia, syncope, vasodilation, bleeding gums, constipation, diarrhea, dysphagia, edema of the tongue, eructation,
flatulence, mouth ulcer, rectal hemorrhage, lymphadenopathy, arthralgia, muscle spasm, tremor, twitch, anxiety, confusion, depression, dizziness, emotional lability, loss of mental acuity, nervousness, paresthesia, somnolence, vertigo, cough, dyspnea, epistaxis, hoarseness, pharyngitis, rhinitis, sinusitis, acne, changes in skin and nail pigmentation, pruritus, rash, sweat, urticaria, amblyopia, hearing loss, photophobia, taste perversion, dysuria, polyuria, urinary frequency, and urinary hesitancy
(Mohammed Ali Al-Bayati Ph.D: - cf www.shirleys-wellness-cafe).
Does it not look like a "medicine" that causes a wide range of illnesses?"The large Anglo-French Concorde randomized trial of zidovudine in asymptomatic HIV-infected individuals shows that there is no significant clinical benefit in terms of survival or disease progression to AIDS or AIDS-related complex (ARC) in those who started zidovudine immediately rather than those who waited for the onset of symptomatic disease. The 1749 participants were followed up for an average of 3 years" (Press Release: Results from Concorde Trial of AZT vs. Placebo. Medical Research Council. 1993 Apr 2; cf David Crowe, June 2001).
Why would a toxic drug that has no significant clinical benefit and that causes so many health complications be used as a medicine?AZT does not prevent the spread of AIDS. AZT does not improve quality of life of AIDS patients. AZT does increase the average life span of AIDS patients. In fact, science shows it to be just the opposite. AZT debilitates the body. AZT weakens or suppresses the immune system and that precipitates more health problems makes the chances of recovery more remote. It does not extend lives, only shorten them. Tragically, AZT can cause AIDS. Yet, there is a medical fraternity who insist that AZT is a medicine!
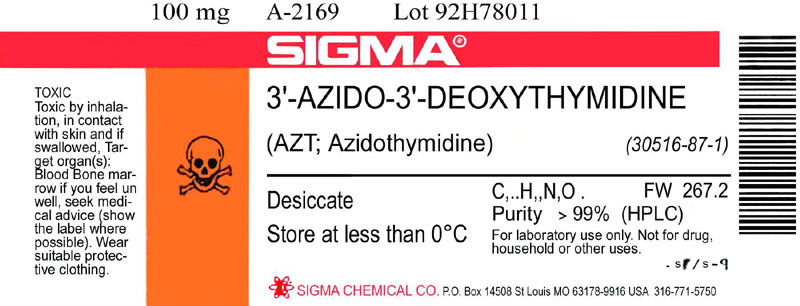
(Click on image to see full size)
THE AZT LABEL - This is what the patient never sees, an actual copy of an AZT label. This label has appeared on bottles containing as little as 25 milligrams, a small fraction (1/20 to 1/50) of some patients' daily prescribed dose.
"WARNING: RETROVIR (ZIDOVUDINE) [AZT] MAY BE ASSOCIATED WITH HEMATOLOGIC TOXICITY INCLUDING GRANULOCYTOPENIA AND SEVERE ANEMIA PARTICULARLY IN PATIENTS WITH ADVANCED HIV DISEASE (SEE WARNINGS). PROLONGED USE OF RETROVIR [AZT] HAS BEEN ASSOCIATED WITH SYMPTOMATIC MYOPATHY SIMILAR TO THAT PRODUCED BY HUMAN IMMUNODEFICIENCY VIRUS. RARE OCCURRENCES OF LACTIC ACIDOSIS IN THE ABSENCE OF HYPOXEMIA, AND SEVERE HEPATOMEGALY WITH STEATOSIS HAVE BEEN REPORTED WITH THE USE OF ANTIRETROVIRAL NUCLEOSIDE ANALOGUES, INCLUDING RETROVIR AND ZALCITABINE, AND ARE POTENTIALLY FATAL (SEE WARNINGS)." - from Glaxo Welcome AZT product information. (See The AZT Label).If it now strikes you that here is a prescription drug that causes AIDS ... well you can't be wrong, especially in consideration of the studies on AZT. It is precription AIDS or as Peter Duesberg calls it AZT AIDS.
AZT therapy was officially indicated only for "AIDS" or "ARC" patients who either had "a history of cytologically confirmed Pneumocystis carinii pneumonia (PCP) or an absolute CD4 (T4 helper/inducer) lymphocyte count of less than 200/mm3 in the peripheral blood before therapy is begun." (Physician's Desk Reference) This changed dramatically when a series of press releases were issued by the National Institute of Allergy and Infectious Diseases (NIAID) and other branches of the Public Health Service (PHS), claiming that AZT was beneficial for "HIV-infected" persons with "mild symptoms of immune system damage" and also for "HIV- infected persons who have not yet developed symptoms" (AZT and Cancer, New York Native, 1987 October 19th, John Lauritsen: see Alberta Reappraising AIDS).
While retorivirals are being cross sold and recommended for use in chemotherapy and chemo drugs being recommended as retrovirals, the National Instutute of Allergy and Infectious Diseases (NIAID) and branches of the PHS have taken the dramatic step to promote AZT as beneficial for "HIV-infected" persons who have not yet developed symptoms. From here, it is not a quantum leap for scientists at such institutions to issue press releases to also say that it is beneficial for people suspected to have cancers but have not yet got their test results to take chemo supplements! So if those type of trends in medical science continue, the day is nigh when it shall be said, "MOM, can I have my chemo supplement please." After all, there are so many products with glycols and parabens.
See also:AIDS Orthodoxy Shaken Up By Maverick Physician
Dr. Jonathan Fishbein's fight for medical ethics in AIDS medicine
In December 2005, GNN's Liam Scheff spoke with NIH whistleblower Dr. Jonathan Fishbein. In an exclusive interview, Fishbein discusses the controversial African AIDS drug trials he exposed, his firing and reinstatement and how medical ethics and the public trust are violated when profit and politics rule the day.The Trouble with Nevirapine
this is a 230-some pages book about the Aids drug Nevirapine by Anthony Brink, an advocate of the High Court of South Africa and convener and chairman of the Treatment Information Group...Study prompts concern about side effects of antiretrovirals
(link no longer active)
Metabolic abnormalities caused by side effects from antiretroviral drugs are becoming increasingly prevalent among Thais living with HIV/Aids, recent studies have found. According to a pilot study by Ramathibodi Hospital's Faculty of Medicine, published in the Journal of the Medical Association Thailand, the long-term toxicity of antiretroviral treatment has become more recognised through a variety of metabolic abnormalities including lipodystrophy, which affects body fat, and dyslipidemia, which affects the blood.
posted by Sepp Hasslberger on Thursday February 10 2005
updated on Friday December 17 2010URL of this article:
http://www.newmediaexplorer.org/sepp/2005/02/10/azt_nevirapine_do_antiretroviral_drugs_cause_aids.htm
Related ArticlesHIV-Aids: A Tragic Error
Recently, a friend from the UK sent a copy of an article published in the Observer, titled: "UK firm tried HIV drug on orphans" which details experiments with toxic AIDS drugs on orphans in New York, involving the British drug giant GlaxoSmithKline. Reading the article I forwarded to some people, a medical doctor friend has the following to say: "I see nothing wrong with this. At least the children received... [read more]
April 12, 2004 - Sepp HasslbergerWangari Maathai: Nobel Calls AIDS 'Weapon Of Mass Destruction'
9 October 2004 - Wangari Maathai, is a Kenyan ecologist and the first African woman to win the Nobel Peace Prize, which she received for her contribution to sustainable development, democracy and peace. Maathai is the founder of the Green Belt Movement, comprised mainly of women, which says it has planted about 30 million trees across Africa. According to a report on the African News24 site titled Nobel winner: Aids... [read more]
October 12, 2004 - Sepp HasslbergerSouth Africa: Traditional Medicine to Fight AIDS, Poverty
The South African Health Minister says that the use of African traditional medicines may eventually replace anti-retrovirals in the treatment of HIV and Aids. Now that is a novel thought. Aids drugs have long been accused of being worse than the disease, their highly toxic shotgun approach kills cells pretty much indiscriminately. A less damaging approach to healing those affected would certainly be welcome. According to this recent article on... [read more]
February 16, 2004 - Sepp HasslbergerHarvard Research in Tanzania Confirms: Multivitamin Slows AIDS Progression
As reported today in the Boston Globe, a research program undertaken by Wafaie Fawzi, Associate Professor of Nutrition and Epidemiology at the Harvard School of Public Health, has found that a multivitamin supplement containing vitamins of the B Complex with C and E was effective in slowing the progression from 'HIV infection' to the clinical picture of AIDS. The study is published in the New England Journal of Medicine and... [read more]
July 01, 2004 - Sepp HasslbergerAZT, Nevirapine - Children In New York Orphanage Given Toxic Drugs
A Catholic orphanage in New York - Incarnation’s Children Center - has allowed its charges, mostly orphans and children removed from their mothers' care, to be used in cruel experiments with drugs that are known to kill most of the patients taking them. This tragedy has taken place under our very noses - we weren't looking. Journalist Liam Scheff has written about this scandal before and you can see that... [read more]
November 05, 2004 - Sepp HasslbergerSelenium Status Is Associated With Accelerated HIV / AIDS
Thanks for sending me this note Harry, then again ethics is not a strong factor amongst the medical Mafiosi - particularly when, egos, greed and wealth have superceded their consciousness. Concern for health, their supposedly original good intentions, have turned to pretense, and have simply become a tool to accomplish their goals incognito... Even more abominable is the zeal with which toxic drugs and immunization are thrust on the sick... [read more]
November 15, 2004 - Chris Gupta

